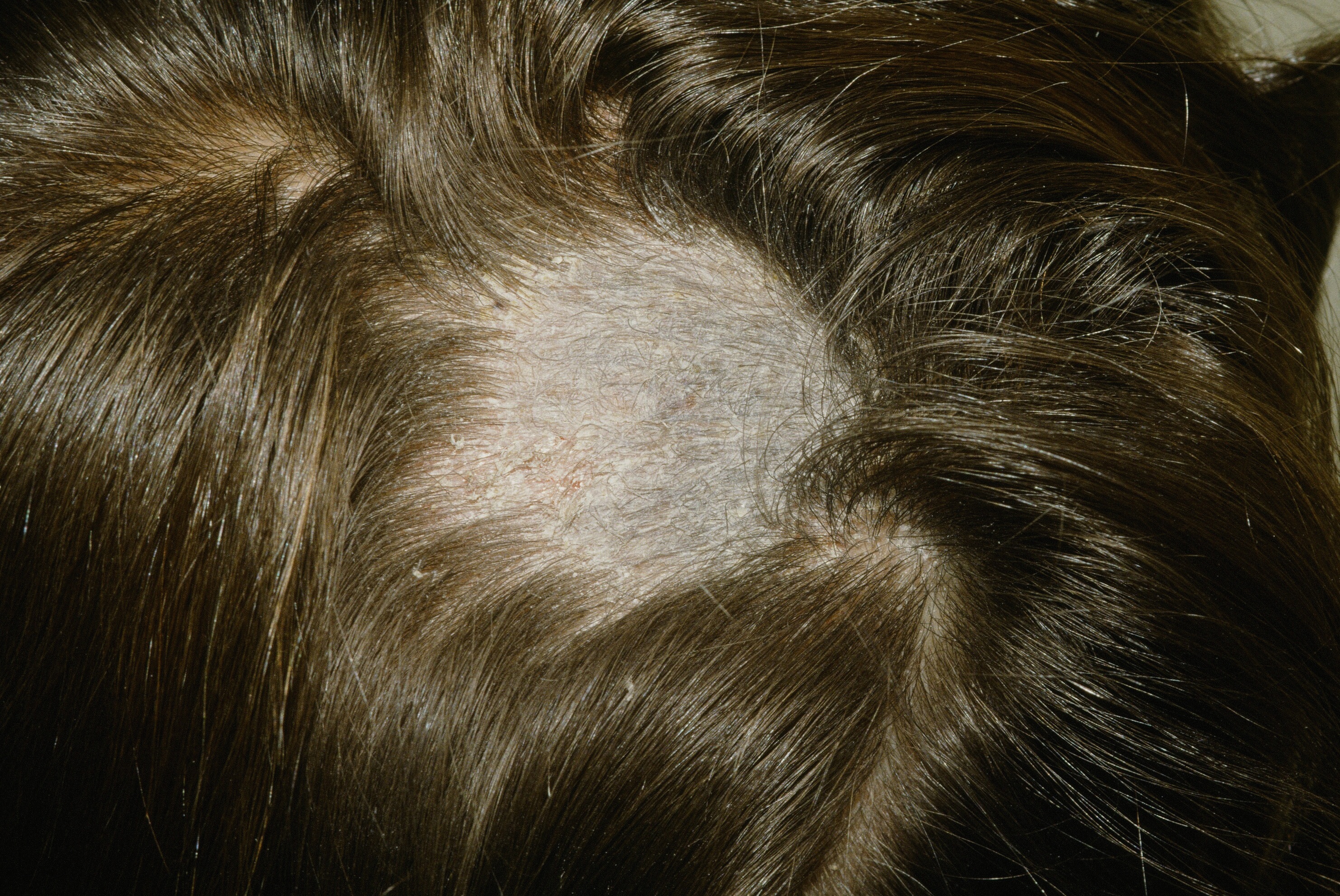
 Note the scaly plaque with hair loss in a child.
Note the scaly plaque with hair loss in a child.
Note the scaly plaque with hair loss in a child.
Tinea Capitis (TC) is a fungal infection of the scalp. It typically affects young, often black children. In North America, Trichophyton tonsurans has replaced M. canis and M. Audouinii as the predominate dermatophyte. Unfortunately, T. tonsurans is Wood's light negative.
There are several clinical patterns including a seborrheic dermatitis-like pattern consisting mainly of scale, a black dot pattern where the hair is broken off at the base resulting in multiple black dots, and a kerion which is where there is so much inflammation, a boggy, swollen nodule forms. The patient may have acquired the organism through contact with other humans, animal, or fomites (inanimate objects). When a kerion is present, lymphadenopathy as well as a secondary eczema are not uncommon (called dermatophytid). Kerion celsi is an inflammatory form of tinea capitis caused by a T-cell–mediated hypersensitivity reaction to the causative dermatophyte.
The clinical presentation may be highly suggestive. Dermoscopy can be helpful to confirm. Look for comma, corkscrew and zig-zag hairs. KOH analysis is rapid, but does not identify the organism and may not be available in all situations. Scalp lesions should be sampled by scalpel scraping, hair pluck, brush or swab as appropriate. Fungal culture is the gold standard for confirmation of the suspected clinical diagnosis but unfortunately, results may take 3-4 weeks.
With regard to the differential of localized hair loss on the scalp, one should consider alopecia areata, trichotillomania, lupus vulgaris, psoriasis and pseudopelade. The likelihood of tinea capitis is extremely high in a child with alopecia and lymphadenopathy.

The black dot pattern where the hair is broken off at the base resulting in multiple black dots.

An inflammatory plaque.
Homepage | Who is Dr. White? | Privacy Policy | FAQs | Use of Images | Contact Dr. White